Quite a few people have been asking about specific injuries and with Euro
2012 heating up we’ve decided to cover injuries to the knee – specifically the
anterior cruciate ligament (ACL), a “favourite” with footballers.
The knee joint is the largest joint in the body, and is made up of: 4
bones (the femur [thigh bone], patella [knee cap], tibia and fibula [your shin
bones]), an extensive network of ligaments and muscles, menisci (that’s the
cartilage) and bursae (for shock-absorption). Just for clarification, your knee
joint should be able to flex (bend) and extend (straighten) and have a small degree of rotation.
 |
| www.healthpages.org ow.ly/bHVLK |
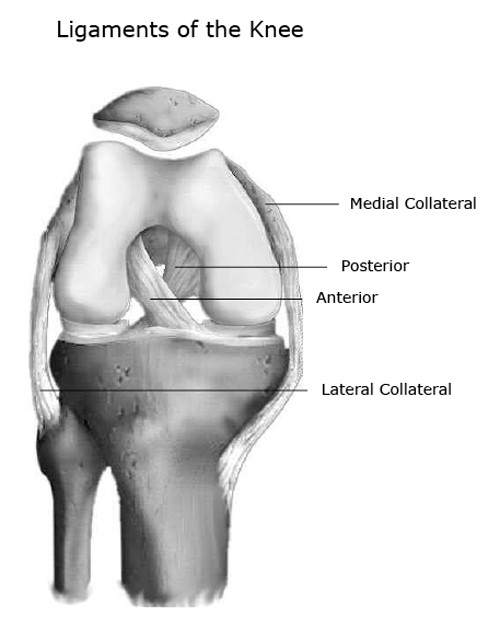
The ligaments provide the joint stability, sort of like straps holding
the bones together. Around the knee there are 4 ligaments – one at each side
(the collaterals), and 2 inside the knee (the cruciates), each having a
specific role in joining the femur to the tibia and fibula, and stabilising the
knee while it bends and straightens.
If one of these ligaments is over-stretched or injured, the knee will
become less stable. Ask most sports people and they’ll tell you that the most frequently
injured ligament is the anterior cruciate ligament (ACL). Its purpose is to limit rotation
and the forward movement of the tibia, so the most common way to injure this ligament is by twisting the knee.
If this happens, your physiotherapist will ask you questions (we love questions) and then examine you in order to classify a sprain as one of 3 grades depending on the extent of the damage. You can expect to experience corresponding symptoms.
- A grade I sprain is where some of the fibres are damaged, and you'll likely feel some pain in the area as well as local swelling and inflammation.
- A grade II sprain is when there is more extensive damage to the fibres. You'll feel moderate pain and moderate joint swelling (this is termed effusion).
- Finally, a grade III sprain is a complete rupture to the ligament - in other words where the ligament has snapped. There is immediate pain and swelling, and you may also hear the knee ‘pop’.
Sometimes an X-ray is taken to rule out
any associated broken bones and the use of MRI scan can be used to identify the
soft tissue injury and ascertain whether any other structures have been affected.
When the swelling settles the most common symptom with grade II and III sprains is joint
instability. You might not experience any symptoms when moving in a
straight line, however, twisting or turning on the
affected leg may cause the knee joint may give way or buckle.
After an ACL injury, some people may be able to return to normal
activities following a period of physiotherapy to help strengthen the muscles
around the joint - these act as the joint stabilisers to "lighten the load" of the ligaments. However,
there is an increased risk of re-injury. Others, especially those
who participate in regular sporting activities which require them to twist and
turn or those who have sustained other soft tissue injuries may require an
operation to ‘repair’ the damaged ligament.
The ligament itself can sometimes heal or be stitched together,
however, in most cases an ACL reconstruction is the only option. This involves
using a tendon (connective tissue which joins muscle to bone) to make a new ACL (more about which ones in a second). Your consultant will normally wait until the swelling has settled and the knee
has regained full range of movement before carrying out any surgery, so physiotherapy can be beneficial to help with this.
 |
| www.ronhebron.com ow.ly/bI0NI |
The operation is a quick key-hole procedure, usually completed at a day
surgery and most often involves the use of your own tendons as the graft
material. The two common tendons used are the hamstring tendon or the
quadriceps tendon (the muscles at the back and front of your thigh respectively), and this is based on the surgeon’s preference. The tendon
that has been removed will re-grow over time but during this process the other
tendons perform the work required.
Following the operation your wound will be covered with a bandage or tubigrip, and you'll need crutches to help you get about (plenty of scope for gleaning some sympathy!) A physiotherapist will be involved immediately following your operation and your rehabilitation will start right away.
In the early stages the main aims
are to reduce the swelling and regain full movement of the joint. You can expect to ditch the crutches after 2-3 weeks, and get back to driving after about a month (but do make sure that you are able to perform
an emergency stop safely and without pain before returning to the roads).
The type
of work you do will affect when you are able to return to work. If you have a
sedentary job then you will be probably be back behind your desk about a month after the
operation. If you perform manual work it will be more like 3 months before
you can return to work. You could take up cycling (on a static bike) and jogging (on a treadmill) about 2-3 months post-op, and your physiotherapist will create a strengthening programme specifically for you as the graft begins to heal, the swelling goes down and your knee begins to move more freely.
 |
| www.getfitfast.com ow.ly/bI1fN |
 |
| www.marathonintense.com ow.ly/bI1uQ |
It is
important to note that the graft is at its weakest in the first 10 weeks or so, just when you're starting to feel great, so don't push it! Unfortunately for all you sporty people, the return to your twisting and turning sports isn't recommended until at least 7 months post-op.
If you think you have injured your ACL, or you have knee problems in general, talk to your physiotherapist or GP for advice. Until then, enjoy Euro 2012!